
http://emedicine.medscape.com/article/1250540-overview#showall
 Total knee arthroplasty. Implanted knee with excellent insertion.
Total knee arthroplasty. Implanted knee with excellent insertion.
 Complications of total knee arthroplasty. Advanced polyethylene wear.
Complications of total knee arthroplasty. Advanced polyethylene wear.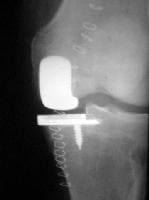 Complications of total knee arthroplasty. With unicompartmental prosthesis, it is vitally important to preserve medial tibial plateau for later revision implantation.
Complications of total knee arthroplasty. With unicompartmental prosthesis, it is vitally important to preserve medial tibial plateau for later revision implantation. Complications of total knee arthroplasty. Previous infection of tibia, with osteomyelitis and tethering of skin to bone.
Complications of total knee arthroplasty. Previous infection of tibia, with osteomyelitis and tethering of skin to bone. Complications of total knee arthroplasty. Dislocation demonstrates poor soft-tissue balancing.
Complications of total knee arthroplasty. Dislocation demonstrates poor soft-tissue balancing. Complications of total knee arthroplasty. Multiple faults ultimately led to excessive wear and osteolysis around stem. Radiograph shows femoral component inserted in flexion and large cysts behind cemented tibial component.
Complications of total knee arthroplasty. Multiple faults ultimately led to excessive wear and osteolysis around stem. Radiograph shows femoral component inserted in flexion and large cysts behind cemented tibial component. Complications of total knee arthroplasty. Postoperative temporary insert.
Complications of total knee arthroplasty. Postoperative temporary insert.
Overview
Total knee replacement (TKA) has become an acceptable method of treating severe arthritis of the knee. The operative procedure must be performed with precise skill and accuracy. Meticulous alignment of the prosthetic components is critical for minimizing complications.[1]
Fine attention to general operating technique with adroit handling of tissues and efficient teamwork (see the image below) can reduce operating time to a minimum and thus avoid exposing the wound for an inordinate amount of time. An experienced, efficient technique also aids in preventing deep venous thrombosis(DVT) and unnecessary scarring and decreases the incidence of many of the complications that are associated with TKA.
Total knee arthroplasty. Implanted knee with excellent insertion.Complications
Complications of total knee arthroplasty (TKA) can be divided into the following 3 categories:
- Complications specific to the operative procedure
- General perioperative complications (including complications of anesthesia)
- Other medical complications (postoperative complications)
Perioperative complications include blood loss, infection, early hemorrhage and wound breakdown, intraoperative fractures, and anesthetic problems, as well ascardiovascular, respiratory, renal, electrolyte, and other medical problems.[2]
Deep venous thrombosis (DVT) is a major danger, particularly if it embolizes to the lung. It is therefore necessary to take appropriate precautions, such as early mobilization, thromboembolic disease stockings, foot pumps, and anticoagulant therapy.
Low-molecular-weight heparin (LMWH) is the drug of choice for DVT prophylaxis. Warfarin, given in a 10-mg dose the night before the operation[3] and subsequently in a daily dose sufficient to keep the international normalized ratio (INR) between 1.5 and 2 for 8 weeks, is also satisfactory.[4] Asymptomatic DVT has been reported in as many as 50-70% of patients who undergo TKA. Postoperative ultrasonography or venography can reveal the presence of thrombi quite successfully.
Older age, greater comorbidity, higher American Society of Anesthesiologists (ASA) classification, and a history of previous disease are associated with an increased risk of cardiac and thromboembolic complications after TKA.[5]
Infection is rare after TKA, occurring in only 1-2.5% of cases. In the early perioperative stages, it should be diagnosed and treated on an urgent basis. Prophylactic antibiotics are used routinely for the first 24 hours.[6]
Neurovascular complications are rare in patients who undergo TKA. The lateral popliteal nerve may be injured in patients with severe valgus deformity. Tourniquet paralysis may also occur, albeit rarely. Major vessel injury may occur in patients undergoing revision procedures or in those rare patients whose anatomy is abnormal.[7, 8]
A study comparing mortality in patients treated by means of TKA with mortality in patients who were awaiting surgical treatment found that the patients in the former group had a significantly greater risk of death at 30 and 90 days after surgery than the patients in the latter group.[9] Increased age was a risk factor for death after the procedure.
A retrospective cohort analysis, using data from 150 patients who underwent unilateral TKA and another 150 who underwent simultaneous bilateral TKA, determined that patients in the bilateral group had 2.1 times higher overall complication rates and increased transfusion rates.[10] Patients with a body mass index (BMI) greater than 30 had higher complication rates than those in the unilateral group, as did those with a preexisting pulmonary disorder. Also demonstrating higher complication rates were patients older than 70 years.
Overall, these study results suggested that age, BMI, and a preexisting pulmonary disorder may result in increased complications.[10]
Long-Term Problems
Major long-term problems that are associated with total knee arthroplasty (TKA) include late infection, wearing of the bearings, and loosening of the prosthesis.[11]Periprosthetic fracture and arthrofibrosis may also occur but are less common.
Component wear
Research is progressing on the wear properties of the ultrahigh-molecular-weight polyethylene used in knee prostheses (see the image below). The coefficient of friction between polyethylene and cobalt-chromium alloy (commonly used for femoral components) has been reported to be between 0.03 and 0.16, with excellent wear rates. The shape and congruency of the bearing surface are important with respect to the contact between the metal component and the polyethylene.
Complications of total knee arthroplasty. Advanced polyethylene wear.
The mobile bearing insert (as opposed to the fixed bearing) is under continuing investigation that focuses on the contact between these 2 surfaces; research efforts are aimed at achieving low contact stresses so as to decrease component wear and further increase range of movement.
Mobile bearing systems have much more contact area; this is seen by some as a disadvantage, because it means that there is more area to undergo wear. Compared with fixed bearings, mobile bearings have significantly reduced upper and lower surface stresses. In addition, unconstrained mobile bearings have a theoretical advantage over semiconstrained mobile bearings (which allow rotation or translation) in that they avoid higher shear stresses; however, they also carry an increased risk of subluxation.
Osteolysis is a major problem with polyethylene and metal wear fragments. The pathology consists of a significant synovitis caused by wear particles in the synovial cavity. In accordance with the Pascal principle, major forces are produced and transmitted throughout the synovial fluid. The wear particles are forced along the lines of least resistance, and the inflamed synovium tracks down the vascular bony foramina around the joint.[12] Severe osteolysis can also occur in pigmented villonodular synovitis and in patients with hemophilia.[13]
Low friction is the aim in all prosthesis design. Therefore, opportunities for improvement include developing finer polishing techniques and using better interface materials. Although ceramics are now commonly used in hip prostheses, they still are used only rarely in knee prostheses. Better grades and design of ceramics will eventually appear.
Technique-related issues
Instrumentation has improved prosthesis implantation techniques substantially, with the result that malalignment and incorrect insertion have been greatly reduced. Computer-assisted surgery is under investigation, and many believe that this approach will decrease the incidence of less-than-satisfactory implantation even further.[14, 15, 16, 17]
A retrospective review study assessed the effect of tibiofemoral alignment, femoral and tibial component alignment, and body mass index (BMI) on implant survival after total knee replacement.[18] The investigators reviewed data from 6070 knees in 3992 patients with a minimum of 2 years of follow-up.
In this study, an increased failure rate was associated with a higher BMI, with failure most likely to occur if the orientation of the tibial component was less than 90° relative to the tibial axis and the orientation of the femoral component was greater than 8° of valgus.[18] Failure was least likely to occur if both the tibial component and the femoral component were in a neutral orientation.
A surgeon embarking on a surgical procedure with a finite lifespan, such as a joint replacement, would do well to keep the next revision procedure in mind.[19] In the primary procedure, it is essential to preserve bone, to refrain from invading the medulla if possible (an advantage of using a stemless prosthesis), and to preserve soft tissues, especially ligaments. Unrecognized medial collateral ligament injuries and failure to manage ligament loss appropriately with additional constraint may result in knee instability and loosening.[20]
Other considerations for discussion include the sacrifice of the posterior cruciate ligament and the place of unicompartmental knee replacement.[21, 22, 23, 24] In a unicompartmental replacement procedure, it is vitally important to preserve the medial tibial plateau for later revision implantation (see the image below). It is also important to select patients who have only unicompartmental degenerative disease.
Complications of total knee arthroplasty. With unicompartmental prosthesis, it is vitally important to preserve medial tibial plateau for later revision implantation.
The benefits of simultaneous versus staged TKA with regard to complication risk continue to be debated in the literature. However, it has been shown that simultaneous unicompartmental knee replacement can be performed without increasing perioperative morbidity or mortality in a younger patient population.[25]
Preoperative assessment and knowledge of previous injuries and operations are important. The image below shows a previous infection of the tibia withosteomyelitis and tethering of the skin to the bone. Skin viability had to be assessed during the procedure to ensure that there would be no breakdown in the postoperative period.
Complications of total knee arthroplasty. Previous infection of tibia, with osteomyelitis and tethering of skin to bone.
Dislocation of a TKA can be seen in the image below, which demonstrates poor soft-tissue balancing. Inadequate spacer insertion, poor ligament balancing, excessive bone resection, or malrotation of the prosthesis can cause this to occur. Many TKAs are inserted in less-than-ideal ways.
Complications of total knee arthroplasty. Dislocation demonstrates poor soft-tissue balancing.
The image below shows a case with many faults that ultimately led to excessive wear and osteolysis around the stem. The femoral component was inserted in flexion, and large cysts are present behind the cemented tibial component. When these technical abnormalities are present in a TKA, they often result in premature failure of the prosthesis and necessitate early revision.
Complications of total knee arthroplasty. Multiple faults ultimately led to excessive wear and osteolysis around stem. Radiograph shows femoral component inserted in flexion and large cysts behind cemented tibial component.
Complications associated with the patellar component are another potential cause of failure after TKA arthroplasty. Such complications include patella tendon avulsion (often associated with a previous high tibial osteotomy); patellofemoral instability due to inadequate soft-tissue balancing; and component failure caused by factors such as a metal-backed component, recurrent instability, loosening, or fracture.[26] Patella clunk is associated with posterior cruciate-sacrificing prosthesis designs in which the peg hits the patella.
The results of one study noted that the use of synthetic mesh for patellar tendon reconstruction is a successful and durable procedure that eliminates the possibility of disease as compared with the use of an allograft.[27]
Whether fixation of components should be done with or without cement is still debated widely. Studies comparing the 2 methods have revealed few, if any, differences.[28] Bioactive coatings such as hydroxyapatite have been used to enhance uncemented fixation, with favorable medium- to long-term results. Prosthetic loosening is the most common cause of long-term failure in TKA, developing as a consequence of osteolysis from wear-particle synovitis.
Infection
Infection is a major disaster in any joint replacement. Accordingly, it must be diagnosed early and treated on an urgent basis.
In the early perioperative period, the key diagnostic distinction is between superficial and deep infection. Blood tests (eg, erythrocyte sedimentation rate [ESR] and C-reactive protein [CRP] level) are not helpful, because they can be affected by the trauma of surgery. Fever is an indication, and the presence of a red, inflamed joint confirms the diagnosis. The synovial white blood cell (WBC) count predicts infection within 6 weeks after primary TKA, with a 94% positive predictive value and a 98% negative predictive value with a cutoff of 27,800 cells/μL.[29]
Saving the prosthesis is possible if early exploration and thorough synovectomy are performed. The chances of preserving the prosthesis are better if it is not cemented.
In late infections, complete removal of the prosthesis, along with all components and cement, is indicated. Measurements of ESR and CRP level are important for diagnosis of chronic infection. Usually, revision of the components is required. A 2-stage revision is best. A postoperative temporary (first-stage) insert can be seen in the image below. It is important to excise all infected tissue; this requires a complete synovectomy and a thorough washout with at least 10 L of isotonic sodium chloride solution.
Complications of total knee arthroplasty. Postoperative temporary insert.
In a study comparing the outcomes achieved with articulating and conventional static spacers after 2-stage reimplantation of TKAs infected with resistant organisms, the investigators noted that whereas outcomes were satisfactory in both groups, the articulating-spacer group had a better functional outcome and a lower incidence of patella infera.[30]
Another study reviewed infected TKA revisions that used an articulating spacer comprising a total condylar component and a meniscal polyethylene insert cemented in place with antibiotic-loaded cement.[31] At an average of 65 months, the Average Knee Society clinical rating for the spacers was 167; the articulating spacer in this study appeared not to require mandatory second-stage surgery.
Other problems
The differential diagnosis of chronic pain in the late postoperative period includes aseptic loosening, arthrofibrosis, sympathetic dystrophy, and, possibly, referred pain from the hip or spine. Arthrolysis may be of benefit with severe arthrofibrosis.
Periprosthetic fracture is a rare complication (occurring in 1-5% of cases) and is usually the result of trauma. Accordingly, it is treated on an individual basis, depending on the site and type of fracture.[32] Other causes of fracture include notching of the femoral component and osteoporosis.[33] In some cases, it may be necessary to insert a large-stem prosthesis. Femoral fracture is the most common type of fracture and usually occurs in the supracondylar region.
No hay comentarios:
Publicar un comentario